

Background: High dose melphalan (HDM) followed by autologous hematopoietic stem cell transplantation (ASCT) is widely used in multiple myeloma (MM) patients as upfront and salvage therapy. However, the safety and efficacy of ASCT in patients with renal insufficiency (RI) is controversial, which have led to an inconsistent arbitrary cut-off for creatinine clearance (CrCl) for performing ASCT. Here we analyzed prospectively the outcomes of MM patients with severe RI who underwent ASCT.
Methods: We enrolled prospectively 50 newly diagnosed MM patients who had a serum CrCl of <40 mL/min at the time of ASCT and an age of up to 65 years. They all received bortezomib-based induction therapy and had achieved at least a partial response before proceeding to ASCT. The recommended dose of melphalan was 140 mg/m2 and it was advised to infuse at least 3 x106/kg autologous CD34+ cells. Consolidation/maintenance post-ASCT was according to the physician's choice. The primary endpoint was transplant related mortality.
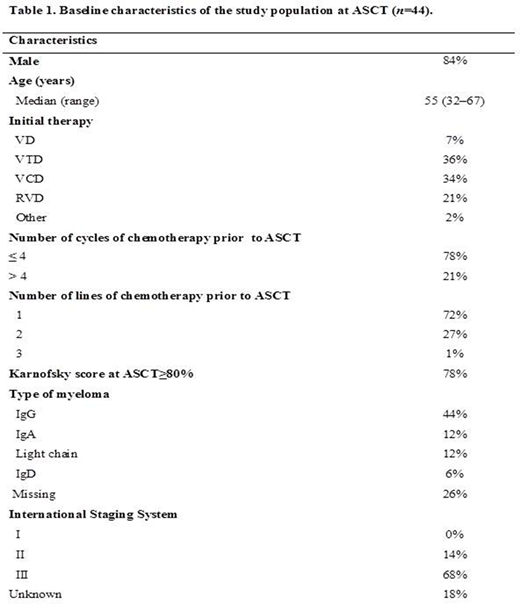
Results: The patients characteristics at enrollment are given in Table 1. We focused on 44 patients who were beyond 3 months post-ASCT. Light chain MM was frequent (12%), 10% had high risk cytogenetics, 36% increased serum LDH and 10% extramedullary disease. Induction chemotherapies included bortezomib plus IMiDs in 25/44 patients with ≥2 lines of chemotherapy in 12/44. The pre-transplant disease status was sCR in =5%, CR in =15%, VGPR in =39%, and PR in =41% of patients. The number of days of cytapheresis was 2 or less in 95% of cases and the median number of CD34+ cells collected was 3.3 x 106 (1.3-9.5). The median time from diagnosis to ASCT was 175 days (103-307). HDM was 140 mg/m2 in 42/44 patients and 200 mg/m2 in 2/44. All, except two, received consolidation post ASCT (34% missing) and 52% had maintenance therapy (all lenalidomide except two receiving bortezomib) and 7% had no maintenance (41% pending).
Toxicity: We observed one death during the first 100 days post-ASCT, secondary to a septic shock on day 42. The median time to neutrophil engraftment was 12 days (9-68) and to platelet engraftment 13 days (10-70). Among patients receiving RBC transfusions (75%) and platelet transfusions (84%), the median number of RBC transfusions was 3 (1-6) and that of platelet transfusions was 3 (1-10). Response: Nine patients (70%) achieved dialysis independence from the time of diagnosis: 13 patients were on dialysis at diagnosis, 5 at the time of ASCT and 4 three months post-ASCT. Renal function improved post-ASCT in 34% of patients, 14% moving from a CrCl of <40 mL/min to 60 mL/min and 20% to above 60 mL/min. No patient experienced worsened renal function following ASCT. At 100 days post-ASCT, the hematological response had improved in 49% of patients, from PR to VGPR (18%), from PR to CR/sCR (11%) and from VGPR to CR/sCR (20%). The best response obtained was 5% PR, 34% VGPR, 47% CR and 11% sCR with one patient relapsing.
Conclusions: In this preliminary analysis, HDM with ASCT proved to be safe and effective in MM patients with RI at transplant. We observed one death among 44 patients within the first 3 months post-ASCT. A more detailed report of the toxicity will be presented during the meeting along with the survival.
Vincent:takeda: Membership on an entity's Board of Directors or advisory committees, Other: Congress support; Celgene: Membership on an entity's Board of Directors or advisory committees, Other: Congress support; janssen: Membership on an entity's Board of Directors or advisory committees, Other: Congress support. Mohty:Jazz Pharmaceuticals: Consultancy, Honoraria, Research Funding, Speakers Bureau; BMS: Consultancy, Honoraria, Research Funding, Speakers Bureau; Novartis: Consultancy, Honoraria, Research Funding, Speakers Bureau; Stemline: Consultancy, Honoraria, Research Funding, Speakers Bureau; Janssen: Consultancy, Honoraria, Research Funding, Speakers Bureau; Celgene: Consultancy, Honoraria, Research Funding, Speakers Bureau; Takeda: Consultancy, Honoraria, Research Funding, Speakers Bureau; GSK: Consultancy, Honoraria, Research Funding, Speakers Bureau; Sanofi: Consultancy, Honoraria, Research Funding, Speakers Bureau; Amgen: Consultancy, Honoraria, Research Funding, Speakers Bureau. Karlin:AbbVie: Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Travel support; Celgene/Bristol-Myers Squibb: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Travel support; Takeda: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Travel support, personal fees; GlaxoSmithKline: Honoraria, Membership on an entity's Board of Directors or advisory committees; Celgene: Other: Personal fees; Sanofi: Honoraria; Amgen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Travel support, personal fees; Janssen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Travel support, personal fees. Morel:Janssen: Honoraria. Rubio:Medac: Consultancy; Gilead: Honoraria; MSD: Honoraria; Novartis: Honoraria; Neovii: Research Funding.

